 ENG
ENG






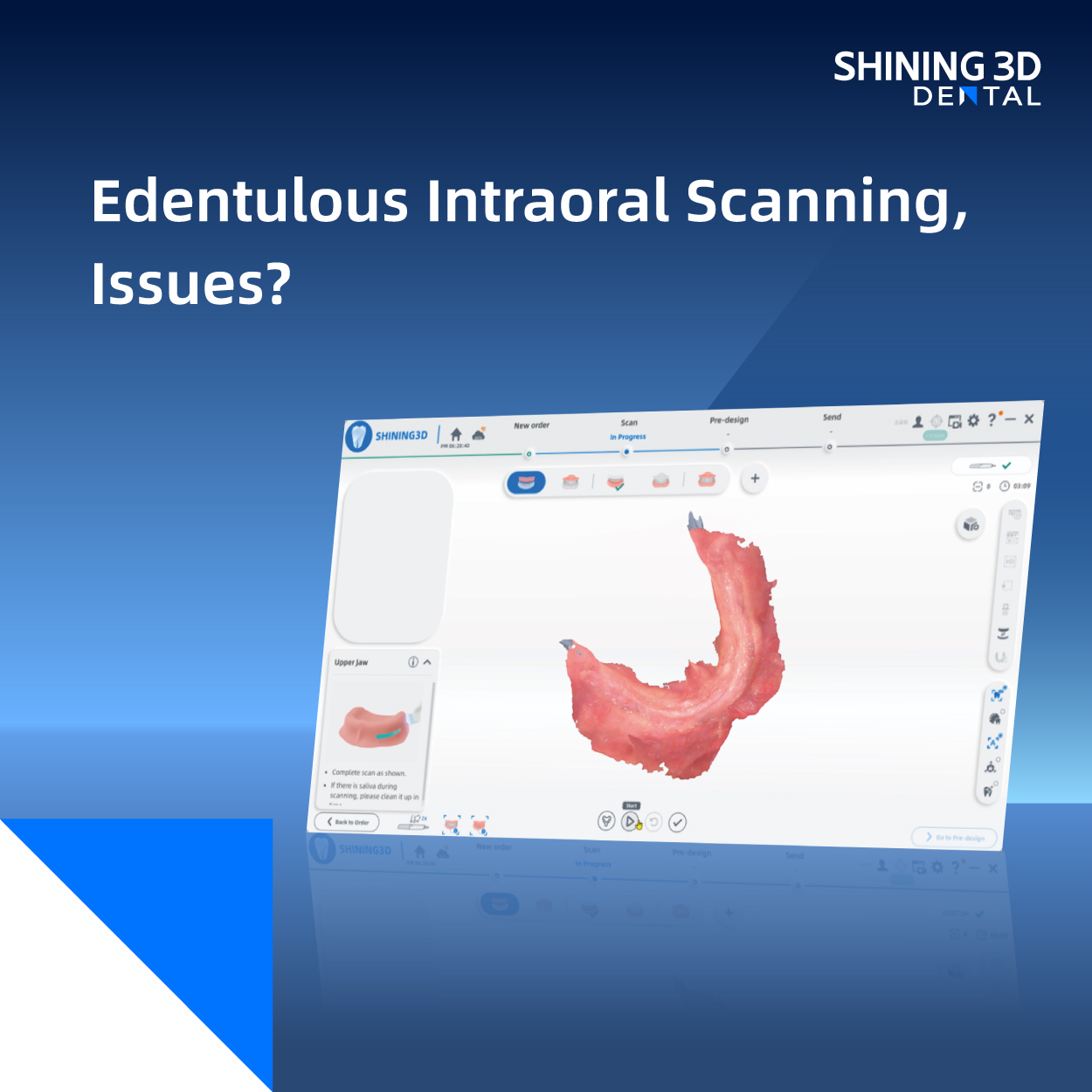
Accurately scanning edentulous arches during the fabrication of complete dentures is a critical yet challenging step, with the quality of digital scans often in question. This article aims to systematically review both clinical and in vitro studies to assess whether intraoral scanners achieve clinically acceptable accuracy when capturing completely edentulous arches for removable complete denture fabrication.

image 1:The scanning of edentulous arches
After conducting an extensive electronic search across major medical databases—PubMed, Scopus, and Web of Science—using pertinent keywords, we identified a total of 334 articles. Following meticulous full-text evaluation, twelve studies (comprising eight clinical trials and four in vitro investigations) met our predefined inclusion criteria. Utilizing the QUADAS-2 tool, we assessed the quality of these studies to ensure rigorous analysis.
Accuracy metrics varied among intraoral scanners, revealing discrepancies particularly in different regions of edentulous arches. Trueness and precision values differed significantly, notably in peripheral borders, the inner seal, and structures like the tongue, muscles and soft palate, which posed challenges for precise digital recording. While scanners performed well in capturing clear anatomic landmarks such as hard tissues with attached mucosa, they exhibited higher discrepancies with mobile and poorly traceable structures.
For complete denture fabrication, achieving an accurate replica of both hard and soft tissues in the denture-bearing area is paramount. Traditional impression-making techniques emphasize either mucostatic or mucodynamic principles, ensuring intimate contact and functional stability of the denture base. The gold standard involves two-stage impression-making using thermoplastic materials for border molding and subsequent impressions material.
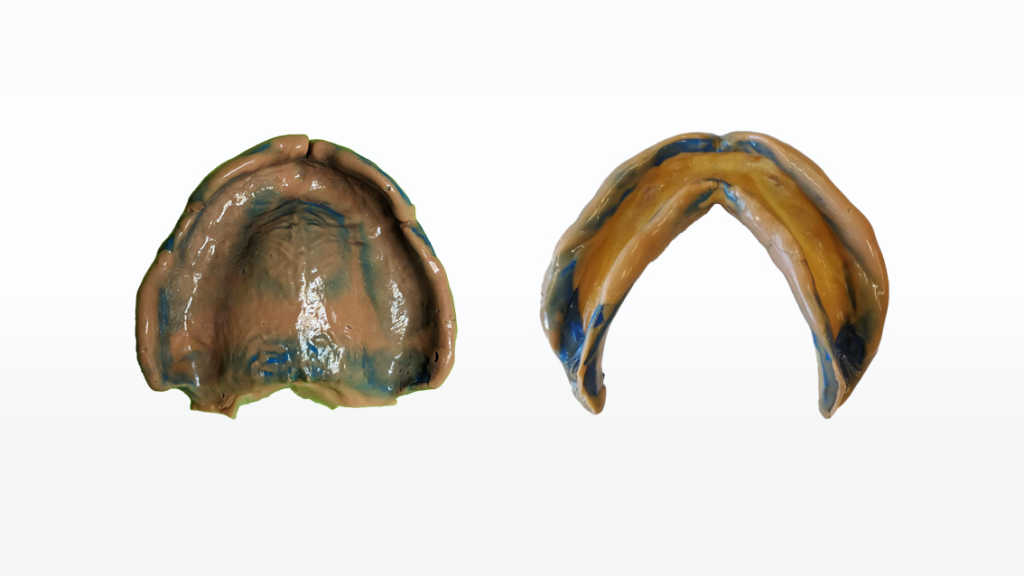
image 2 and 3 : Physical impression of upper and lower jaws
Image Credit:clinical work by Mark Samuel Chan DD, Toronto Canada
In full arch scanning of implants, additional challenges arise beyond traditional impression-making issues. Specifically, stitching together scan bodies that are spaced far apart can reduce the accuracy and precision of the scanned arch. Misalignment or discrepancies between scan segments can lead to a less accurate digital model, affecting the fit and function of the final prosthetic.
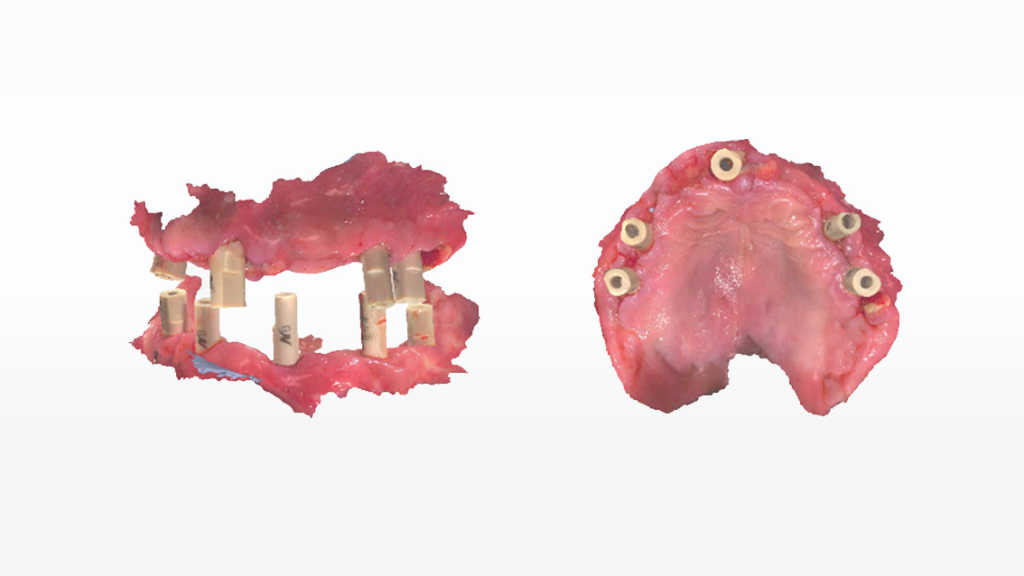
image 4 and 5 : The intraoral scan data (All-on-X)
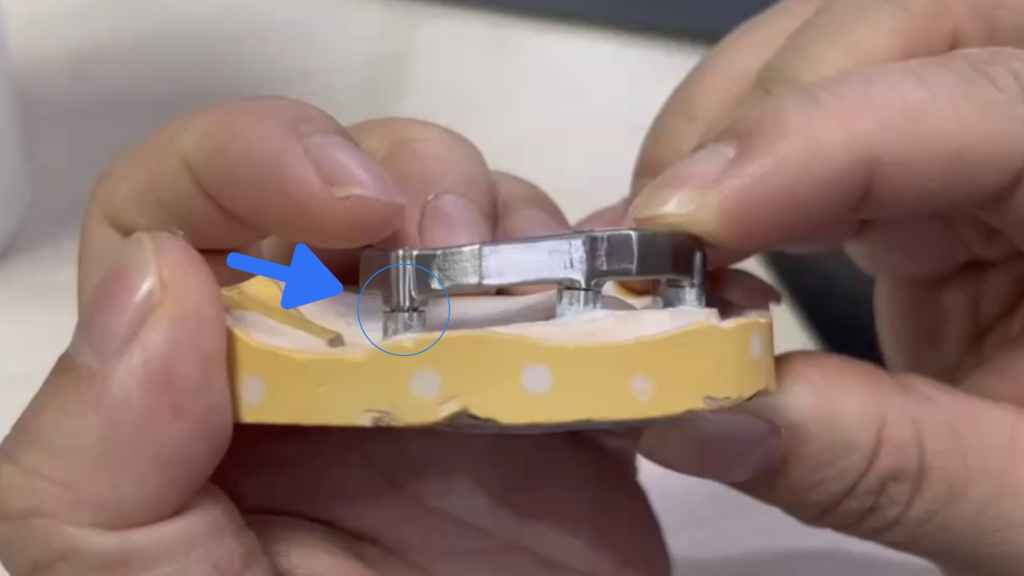
image 6 : Traditional precision issue of passive fit
In contrast, intraoral scanners offer advantages such as reduced patient discomfort and seamless data transfer to laboratories, though challenges persist in capturing the intricate anatomy of edentulous jaws, particularly areas with movable mucosa and variable textures. Techniques to improve scanning reliability include modifying mucosal landmarks and optimizing scanning protocols to enhance accuracy during stitching processes.
While intraoral scanners show promise in simplifying the impression-making process for fixed and implant-supported prostheses, their efficacy in recording edentulous arches remains a topic of ongoing investigation. Case reports highlight the feasibility of digital workflows, yet discrepancies in scanning mobile mucosal surfaces suggest room for improvement. Standardizing quantification methods for deviations and assessing their clinical impact on denture fit and comfort are crucial for advancing digital scanning technologies in prosthodontics.
In conclusion, while intraoral scanners demonstrate clinically acceptable accuracy in capturing edentulous arches, especially for fixed and implant-supported prostheses, challenges persist in optimizing scans of mobile mucosa and unfavorable ridge anatomy. Case selection and protocol refinement are essential steps towards maximizing the potential of digital intraoral scanning in complete denture fabrication